





File. Neurology research, conceptual image. Scientist viewing a patient’s brain scan during clinical tests in the lab
U.S. officials have approved another Alzheimer’s drug that can modestly slow the disease, providing a new option for patients in the early stages of the incurable, memory-destroying ailment.
The Food and Drug Administration approved Eli Lilly’s Kisunla on Tuesday for mild or early cases of dementia caused by Alzheimer’s. It’s only the second drug that’s been convincingly shown to delay cognitive decline in patients, following last year’s approval of a similar drug from Japanese drugmaker Eisai.
The delay seen with both drugs amounts to a matter of months — about seven months, in the case of Lilly’s drug. Patients and their families will have to weigh that benefit against the downsides, including regular IV infusions and potentially dangerous side effects like brain swelling.
Physicians who treat Alzheimer’s say the approval is an important step after decades of failed experimental treatments.
“I’m thrilled to have different options to help my patients,” said Dr. Suzanne Schindler, a neurologist at Washington University in St. Louis. “It’s been difficult as a dementia specialist — I diagnose my patients with Alzheimer’s and then every year I see them get worse and they progress until they die.”
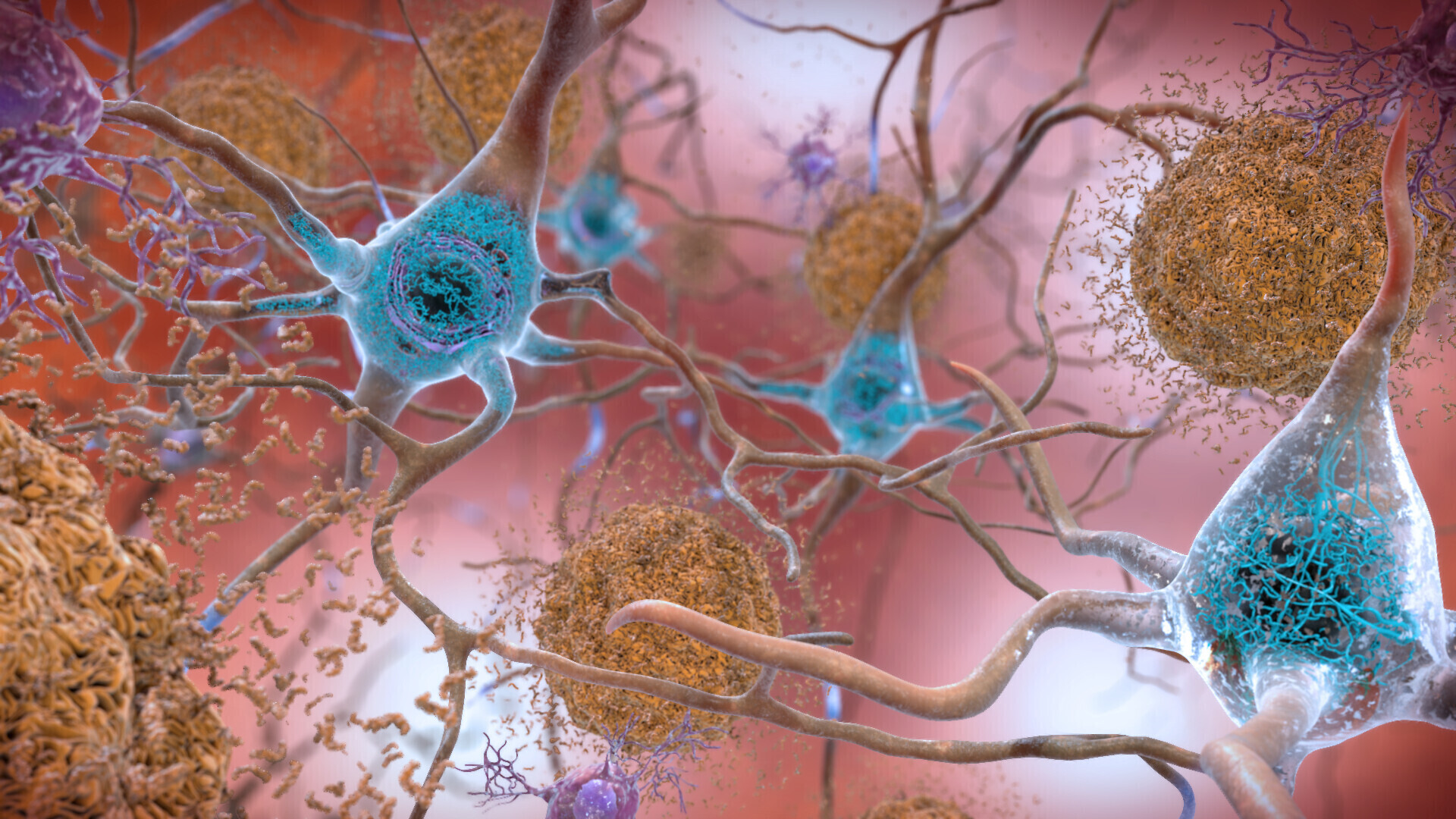
Both Kisunla and the Japanese drug, Leqembi, are laboratory-made antibodies, administered by IV, that target one contributor to Alzheimer's — sticky amyloid plaque buildup in the brain. Questions remain about which patients should get the drugs and how long they might benefit.



The new drug's approval was expected after an outside panel of FDA advisors unanimously voted in favor of its benefits at a public meeting last month. That endorsement came despite several questions from FDA reviewers about how Lilly studied the drug, including allowing patients to discontinue treatment after their plaque reached very low levels.
Costs will vary by patient, based on how long they take the drug, Lilly said. The company also said a year’s worth of therapy would cost $32,000 — higher than the $26,500 price of a year’s worth of Leqembi.
The FDA’s prescribing information tells doctors they can consider stopping the drug after confirming via brain scans that patients have minimal plaque.
More than 6 million Americans have Alzheimer’s. Only those with early or mild disease will be eligible for the new drug, and an even smaller subset are likely to undergo the multi-step process needed to get a prescription.
The FDA approved Kisunla, known chemically as donanemab, based on results from an 18-month study in which patients given getting the treatment declined about 22% more slowly in terms of memory and cognitive ability than those who received a dummy infusion.
The main safety issue was brain swelling and bleeding, a problem common to all plaque-targeting drugs. The rates reported in Lilly's study — including 20% of patients with microbleeds — were slightly higher than those reported with competitor Leqembi. However, the two drugs were tested in slightly different types of patients, which experts say makes it difficult to compare the drugs' safety.
Kisunla is infused once a month compared to Leqembi’s twice-a-month regimen, which could make things easier for caregivers who bring their loved ones to a hospital or clinic for treatment.
“Certainly getting an infusion once a month is more appealing than getting it every two weeks,” Schindler said.
Lilly's drug has another potential advantage: Patients can stop taking it if they respond well.
In the company’s study, patients were taken off Kisunla once their brain plaque reached nearly undetectable levels. Almost half of patients reached that point within a year. Discontinuing the drug could reduce the costs and safety risks of long-term use. It's not yet clear how soon patients might need to resume infusions.
Logistical hurdles, spotty insurance coverage and financial concerns have all slowed the rollout of competitor Leqembi, which Eisai co-markets with U.S. partner Biogen. Many smaller hospitals and health systems aren’t yet setup to prescribe the new plaque-targeting Alzheimer's drugs.
First, doctors need to confirm that patients with dementia have the brain plaque targeted by the new drugs. Then they need to find a drug infusion center where patients can receive therapy. Meanwhile, nurses and other staff must be trained to perform repeated scans to check for brain swelling or bleeding.
“Those are all things a physician has to have set up," said Dr. Mark Mintun, who heads Lilly’s neuroscience division. "Until they get used to them, a patient who comes into their office will not be offered this therapy.”


